Making and Response to a Referral
Within one working day of a referral being received a local authority social worker should make a decision about the type of response that is required.
1. Making a Referral - Overview
1.1 Professionals, employees, managers, helpers, carers and volunteers in all agencies must make a referral to Children’s Social Care if it is believed or suspected that:
- A child is suffering or is likely to suffer Significant Harm, or
- A child would be likely to benefit from family support services with the agreement of the person who has Parental Responsibility.
2. Duty to Refer
2.1 When there are concerns about Significant Harm, then the referral must be made immediately. The greater the level of perceived risk, the more urgent the action should be. The suspicion or allegation may be based on information, which comes from different sources. It may arise in the context of an Early Help Assessment. It may come from a member of the public, the child concerned, another child, a family member or a professional. It may relate to a single incident or an accumulation of lower level concerns.
2.2 The information may also relate to harm caused by another child, in which case both children, i.e. the suspected perpetrator and victim, must be referred to Children’s Social Care.
2.3 The suspicion or allegation may relate to a parent, professional, volunteer or anyone caring for or working with the child - if so, see also Allegations and Concerns against Staff, Carers or Volunteers Procedure.
2.4 A safer referral must be made even if it is thought that Children’s Social Care may already be involved with the child/family.
3. Urgent Medical Treatment
3.1 If the child is suffering from a serious injury or requires treatment, medical attention must be sought immediately by calling an ambulance or taking the child to the Accident and Emergency Department of the local hospital. The duty Consultant Paediatrician must be informed of the nature of the concerns and a referral must be made in accordance with this procedure as soon as practicably possible.
4. Ensuring Immediate Safety
4.1 The safety of children is paramount in all decisions relating to their welfare. Any action taken by a professional should ensure that no child is left in immediate danger.
4.2 When considering whether immediate action is required to protect a child, all agencies should also consider whether action is required to safeguard and protect the welfare of any other children in the same household or related to the household or the household of an alleged perpetrator or elsewhere e.g. a work environment such as a school.
4.3 The law empowers anyone who has care of a child to do all that is reasonable in the circumstances to safeguard her/his welfare.
4.4 A teacher, foster carer, child-minder or any professional should take all reasonable steps to offer a child immediate protection from an abusive parent / carer.
4.5 Where abuse is alleged, suspected or confirmed in children admitted to hospital, they must not be discharged until a referral has been made to the relevant Children’s Social Care in accordance with this procedure and a decision made as to the need for immediate protective action.
5. Confidentiality
5.1 The safety and welfare of the child overrides all other considerations, including the following:
- Confidentiality;
- The gathering of evidence;
- Commitment or loyalty to relatives, friends or colleagues.
5.2 For further details, see Information Sharing Guidance
5.3 The overriding consideration must be the protection of the child - for this reason, absolute confidentiality cannot and should not be promised to anyone.
5.4 Individual members of the public who make a referral may prefer not to give their name or alternatively they may disclose their identity, but not wish for it to be revealed to the parents/carers of the child concerned.
5.5 Wherever possible, Children’s Social Care workers receiving referrals from members of the public should respect the referrer’s request for anonymity. However, referrers should not be given any guarantees of confidentiality, as there are certain limited circumstances in which the identity of a referrer may have to be given e.g. the Criminal or Family Court arena. The referrer’s request for anonymity must be recorded.
5.6 A professional making a referral should not expect anonymity. However, in exceptional circumstances where disclosure to third parties could endanger the referrer, managers should assess risk and if necessary agree anonymity at this juncture. Professionals making referrals cannot choose to remain anonymous however It is acknowledged that on occasions a professional may need to make a referral as a result of something they have seen, heard or been told in their private life. In this situation it is important they are able to remain anonymous if needed in order to ensure the safety of themselves or their families. Such a referral should be made by the usual route and in making this referral the individual is responsible for ensuring they adhere to any expected code of professional conduct.
6. Child’s Voice and Expressed Wishes
6.1 If the child makes an allegation or discloses information which raises concern about Significant Harm, the initial response should be limited to listening carefully to what the child says so as to:
- Clarify the concerns;
- Offer reassurance about how (s)he will be kept safe; and
- Explain that the information will be passed to Children’s Social Care and/or the Police.
6.2 If a child is freely recalling events, the response should be to listen, rather than stop the child; however, it is important that the child should not be asked to repeat the information to a colleague or asked to write the information down.
6.3 If the child has an injury but no explanation is volunteered, it is acceptable to enquire how the injury was sustained. However, the child must not be pressed for information, led or cross-examined or given false assurances of absolute confidentiality. Such well-intentioned actions could prejudice police investigations, especially in cases of Sexual Abuse.
6.4 A record of all conversations, including the timings, the setting, those present, as well as what was said by all parties and actions must be kept.
6.5 It is very important to ensure that all conversation with a child is recorded throughout the process. If a criminal investigation proceeds, failure to follow the guidance in relation to listening and recording information provided by a child could lead to conflict and the credibility of the child's account being undermined at court.
6.6 No enquiries or investigations may be initiated without the authority of Children’s Social Care or the Police.
6.7 If the child can understand the significance and consequences of making a referral, he/she should be asked her/his views by the referring professional.
6.8 Whilst the child’s views should be considered, it remains the responsibility of the professional to take whatever action is required to ensure the safety of that child and any other children.
6.9 Where the child expresses a wish for his or her parents not to be informed, their views should be taken seriously and a judgement made based on the child’s age and understanding, as to whether the child’s wishes should be followed.
7. Parent / Carer Consultation and Consent
7.1 Professionals should seek to discuss concerns with the family and, where possible seek the family’s consent to making a referral unless this may, either by delay or the behavioural response it prompts or for any other reason, place the child at increased risk of Significant Harm.
7.2 Where a parent/carer has consented to a referral, this must be recorded and confirmed on the Safer Referral Form (which can be downloaded on this website).
7.3 If, having taken full account of the parent’s wishes, it is still considered that there is a need for a referral, the reason for proceeding without parental agreement must be recorded on the Safer Referral Form and the parent should be contacted by the referring professional to inform her/him that after considering their wishes, a referral has been made.
7.4 Concerns must not be discussed with parents/carers before making a referral where:
- Discussion would put a child at risk of significant harm
- Discussion would impede a Police investigation or social work enquiry
- Sexual abuse is suspected
- Organised or multiple abuse is suspected
- Fabricated or induced illness is suspected
- Contact with the parents/carers would place you or others at risk
- Honour Based Violence is suspected
- Forced Marriage is suspected
8. Making a Referral
8.1 Referrals must be made in one of the following ways:
- By contacting the relevant Children’s Social Care office (See Local Contacts - select the relevant local authority logo).
- In an emergency outside office hours, by contacting Children’s Social Care Emergency Duty Team (EDT) by Telephone (See Local Contacts - select the relevant local authority logo) or the Police (101).
- All professionals must confirm verbal and telephone referrals with the Safer Referral Form within 48 hours of being made, this can be done via secure email address or post.
8.2 In the vast majority of cases, there will have been a history of additional needs prior to a child being referred to Children's Social Care. It is the responsibility of all agencies working directly with children and families to attempt to respond to these needs at an early stage under Early Help. For this reason, it is expected that all referrals to Children’s Social Care made during office hours from agencies working directly with children and families should be accompanied by a completed Early Help Assessment and evidence of Early Help activity undertaken were possible.
8.3 In the event that an agency does not agree with the response and decisions about the referral by Children’s Social Care, the referring agency should discuss their concerns directly with the manager making the decision, in the first instance to seek resolution.
8.4 Professionals in most agencies should have internal procedures, which identify a Designated Senior Persons or Named Professionals - Managers or Staff, who are able to offer advice on child protection matters and decide upon the necessity for a referral.
8.5 Arrangements within an agency may be that a designated person makes the referral. However, if the designated or named person is not available, the referral must still be made without delay.
8.6 A referral or any urgent medical treatment must not be delayed by the unavailability of designated or named professionals.
9. How Referrals will be received
9.1 Children’s Social Care will ensure that a duty worker is available to receive child protection referrals; outside normal working hours, the Emergency Duty Team will receive referrals.
9.2 Children’s Social Care will deal with the referral in accordance with the Local Common Assessment Framework, Local Threshold Document the Framework of Assessment (Threshold document) (Practitioners working in Middlesbrough should consult the Middlesbrough Threshold of Need Document) and the Assessment Framework Triangle in Working Together and determine whether a referral should be responded to on the basis that the child is in need of support under section 17 of the Children Act 1989 or in need of protection under Section 47 of the Children Act 1989.
9.3 The worker receiving a referral will establish:
- The nature of the concern;
- How and why it has arisen;
- What the child’s and family’s needs appear to be;
- Whether the concern involves any risk of Significant Harm;
- Whether there is any need for any urgent action to protect the child, any other child in the same household or any child in contact with an alleged perpetrator.
9.4 To do so, the worker receiving the referral will usually discuss the case with the referrer and in doing so, will:
- Give their name and designation;
- Help the referrer to give as much relevant information as possible
- Clarify information that the referrer is reporting directly and information that has been obtained from a third party;
- Discuss whether there are concerns about maltreatment and if so, what is their foundation;
- Clarify who has and who has not been told about the referral;
- Clarify the whereabouts of the child;
- Discuss whether it may be necessary to consider taking urgent action to ensure the safety of the child or any other child in the same household or who is in contact with an alleged perpetrator;
- Agree how to re-contact the referrer if further clarification is required;
- Clarify the extent to which the referrer’s anonymity can be maintained (if this is a non-professional referrer);
- Clarify expectations about how and when feedback is to be given.
9.5 Referrers should be asked specifically if they hold any information about difficulties being experienced by the family/household due to domestic violence and abuse, mental illness, substance misuse, and/or learning difficulties.
9.6 Children’s Social Care should decide upon a course of action. And acknowledge receipt of a Safer Referral Form within one working day.
9.7 Parents should be informed of the referral and their permission sought to share information with other agencies unless to do so would:
- Impact any investigations or enquiries;
- Place the child’s welfare and/or safety at risk;
- Cause concern that the child would be at risk of further Significant Harm.
9.8 In these circumstances, a manager from Children’s Social Care may decide to consult other relevant agencies without seeking parental consent. Any such decision must be recorded with reasons.
10. Where there is or may be a crime committed
10.1 If the referral relates to a situation in which a crime has or may have been committed, including sexual or physical assault or neglect, the worker receiving the referral must discuss the referral with the Police Protecting Vulnerable People Unit (PVP Unit) at the earliest opportunity. The PVP, in consultation with Children’s Social Care and any other agencies involved with the child, must consider whether there should be a criminal investigation and/or a Children’s Social Care led intervention.
10.2 Whilst the responsibility to instigate criminal proceedings rests with the Police, they should consider the view expressed by other agencies.
11. Cross Boundaries Referrals
11.1 If the referral relates to a child who is temporarily visiting the area of another local authority or in a hospital or Looked After outside of the local area, the local authority/Police for the area where the child actually is at the time have prime responsibility for an initial response to the referral.
11.2 The referral should be passed to that authority immediately for them to follow the necessary procedures and to undertake a Section 47 Enquiry and/or take any immediate protective action that is necessary. They will be responsible for liaising with any other Children’s Social Care as necessary.
11.3 For further information related to: Cross Boundaries Procedure
12. Pre-birth Referrals
12.1 Where agencies or individuals anticipate that an unborn baby may be at risk of Significant Harm, a referral to Children’s Social Care must be made in accordance with Safeguarding the Unborn Baby procedure.
13. Local Information
13.1 If you wish to make a referral to one of the following local authorities click on the name of that authority and you will be directed appropriately:
North Tees CHub (Hartlepool & Stockton-on-Tees)
South Tees MACH (Middlesbrough & Redcar & Cleveland)
14. Response to a Referral - Overview
14.1 Once the referral has been accepted by local authority children’s social care the lead profession role falls to a social worker. The social worker should clarify with the referrer, when known, the nature of the concerns and how and why they have arisen. Within one working day of a referral being received a local authority social worker should make a decision about the type of response that is required. This will include determining whether:
- the child requires immediate protection and urgent action is required;
- the child is in need and should be assessed under section 17 of the Children Act 1989;
- there is reasonable cause to suspect that the child is suffering or likely to suffer significant harm and whether enquiries must be made and the child assessed under section 47 of the Children Act 1989;
- any services are required by the child and family and what type of services; and
- further specialist assessments are required in order to help the local authority to decide what further action to take.
15. Action to be taken
15.1 The child and family must be informed of the action to be taken.
15.2 Local authority children’s social care should see the child as soon as possible if the decision is taken that the referral requires further assessment.
15.3 Where requested to do so by local authority children’s social care, professionals from other parts of the local authority such as housing and those in health organisations have a duty to cooperate under section 27 of the Children Act 1989 by assisting the local authority in carrying out its children’s social care functions.
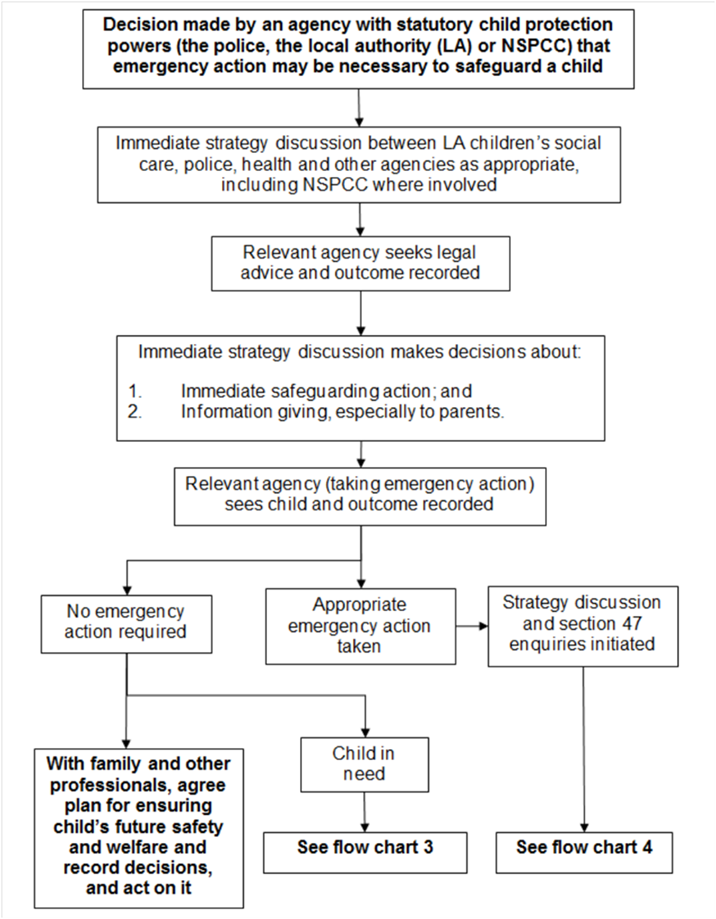
16. Immediate Protection
16.1 Where there is a risk to the life of a child or a likelihood of serious immediate harm, local authority social workers, the police or NSPCC should use their statutory child protection powers to act immediately to secure the safety of the child.
16.2 If it is necessary to remove a child from their home, a local authority must, wherever possible and unless a child’s safety is otherwise at immediate risk, apply for an Emergency Protection Order (EPO). Police powers to remove a child in an emergency should be used only in exceptional circumstances where there is insufficient time to seek an EPO or for reasons relating to the immediate safety of the child.
16.3 An EPO made by the court given authority to remove a child and places them under the protection of the applicant.
16.4 When considering whether emergency action is necessary an agency should always consider the needs of other children in the same household or in the household of an alleged perpetrator.
16.5 The local authority in whose area a child is found in circumstances that require emergency action (the first authority) is responsible for taking emergency action.
16.6 If the child is looked after by or the subject of a child protection plan in another authority, the first authority must consult the authority responsible for the child. Only when the second local authority explicitly accepts responsibility (to be followed up in writing) is the first authority relieved of its responsibility to take emergency action.
16.7 For further guidance on EPO's see chapter 4 of Court orders and pre-proceedings: For local authorities (April 2014)
17. Action taken when a child is referred to local authority children's social care services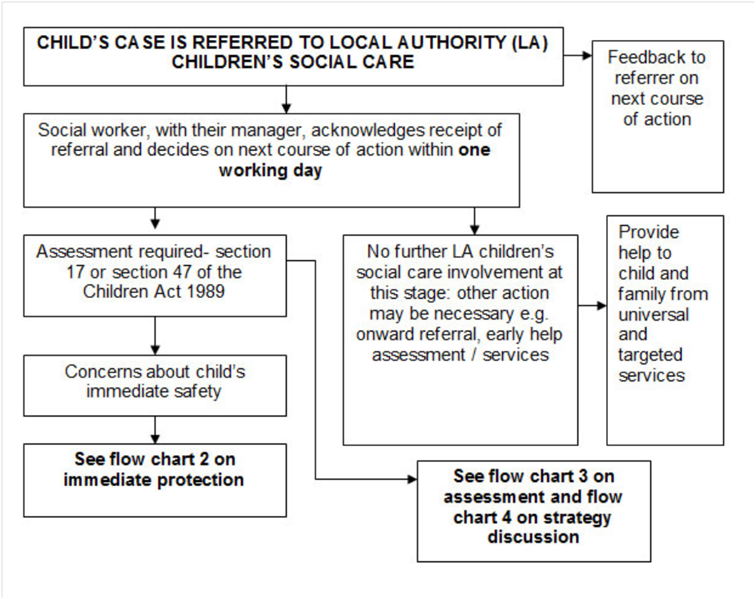

18. Multi-Agency Working
18.1 Planned emergency action will normally take place following an immediate strategy discussion. Social Workers, the police or NSPCC should:
- Initiate a strategy discussion to discuss planned emergency action. Where a single agency has to act immediately, a strategy discussion should take place as soon as possible after action has been taken;
- see the child (this should be done by the practitioner from the agency taking the emergency action) to decide how best to protect them and whether to seek an EPO; and
- wherever possible, obtain legal advice before initiating legal action, in particular when an EPO is being sought.
19. Flowchart: Immediate Protection